")
Pregnancy will never be easy and will always be one of the most painful experiences a woman can have, but it is also one of the most precious times of her life. Before we tackle all about anti-, intra-, and postpartum and neonatal care, let’s first understand the reproductive system that made this possible.
Uterus

The uterus is a pear-shaped organ that is essential for menstruation, conception, and pregnancy. It is hollow and muscular, and it resides within your pelvis between your rectum and bladder.
The uterus is anatomically composed of the endometrium, which is the most inner layer of the uterus, the myometrium, which is the second layer of the uterus, and the perimetrium, which encases the entire organ; and two major sections, which are the body or corpus of the uterus and the cervix, which is the lower part of it.
The uterus is an internal organ of female reproduction that enlarges to the point where it becomes an abdominal organ around the 12th week of pregnancy to accommodate the fetus’s growth.
The cervix shields the internal environment of female reproduction from the outside world; during pregnancy, the cervix safeguards the fetus.
Vagina
This internal reproductive organ connects the external structures of the female reproductive system to the interior female reproductive organs and structures. The vaginal canal is a muscular canal surrounded by nerves and mucous membranes. It connects the uterus and cervix to the outer world, making menstruation, intercourse, and childbirth possible. Because it creates high acidity, it protects against infection during pregnancy; also, the vaginal becomes more vascular during pregnancy.
The Fallopian Tubes
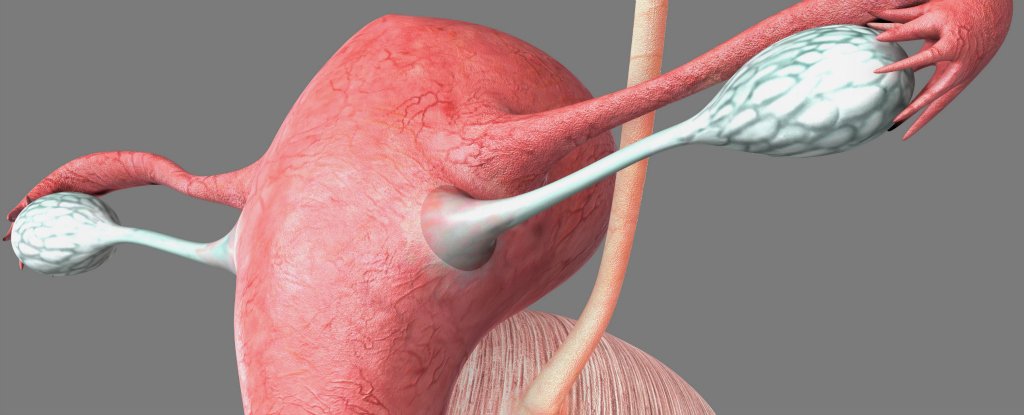
They are vital components of the female reproductive system. The fallopian tubes are the site of fertilization; the fertilized ovum goes from the trumpet-like ampulla of the fallopian tube to the uterus after about 4 days, with the exception of ectopic pregnancies, which abnormally keep the fertilized ovum in the fallopian tube.
The fallopian tubes are also referred to as the oviducts or the uterine tubes. Permanent contraception or sterilization can be achieved by medical treatments that restrict the fallopian tubes.
Ovaries
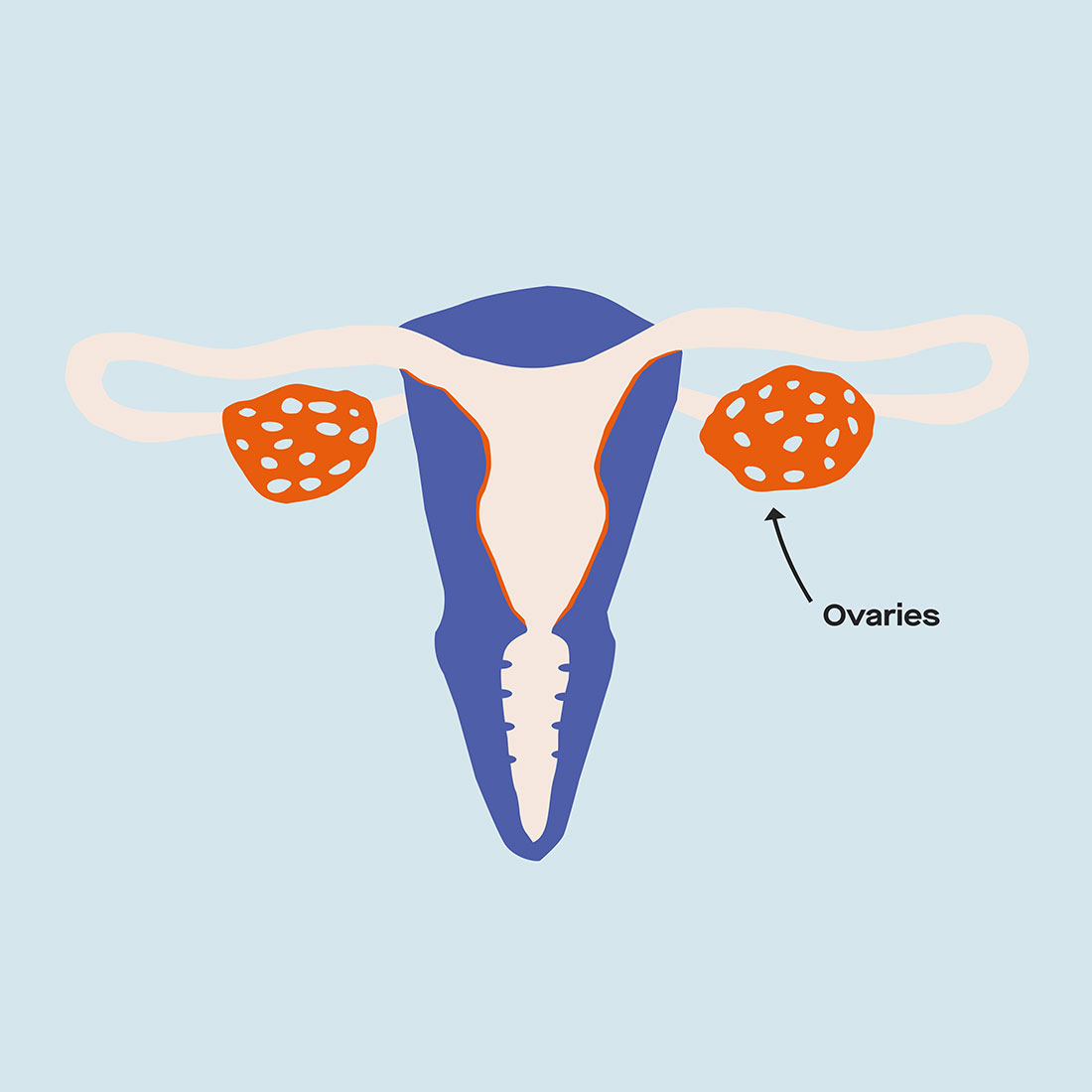
The female gonads, or ovaries, are the primary female reproductive organs. These glands serve three functions: they secrete hormones, safeguard the eggs that a female is born with, and release eggs for possible fertilization. Unlike other reproductive organs, the ovaries function as both an endocrine and a reproductive organ. As an endocrine organ, the ovaries produce hormones such as progesterone and estrogen. These hormones are essential for a woman’s menstrual cycle, breast development, and the continued retention of a growing fetus throughout pregnancy.
Bony Pelvis

The pelvis is a basin-shaped set of bones in the human anatomy that links the trunk and the legs, supports and balances the body, and holds and supports the intestines, urine bladder, and internal sex organs.
The bony pelvis, which consists of two innominate bones, the sacrum, and the coccyx, and which, unlike other elements of the human skeletal system, becomes more malleable and adaptable during labor and vaginal birth to assist the transfer of the fetus to the external world.
Conception
Conception and fertilization are intricate processes involving cellular division, gametogenesis, and chromosomal organization. Mitosis and meiosis generate a single cell during fertilization; gametogenesis is the generation of a single male sperm or a single female egg, each of which has 23 pairs of chromosomes and which, following fertilization, forms the zygote with 46 pairs of chromosomes. Males and females each have 23 pairs of chromosomes, two of which are sexually assigned autosomes and the rest are not. Males have XY chromosomal arrangements, while females have XX female chromosomal arrangements.
Examining the Client’s Psychosocial Reactions to Pregnancy
In addition to assessing the client’s physiological changes and responses to pregnancy, the registered nurse assesses the client’s psychosocial responses to pregnancy, including those associated with the mother’s response to and thoughts of the pregnancy, the father’s reaction to and thoughts of the pregnancy, the coping mechanisms used by the mother and father as they deal with this developmental and maturation change, and the parents’ emotional preparedness for the pregnancy.
It is estimated that over 50% of all pregnancies are unplanned, and single moms, especially adolescent mothers, frequently become pregnant. Some moms and fathers are able to adapt to and welcome an unexpected pregnancy, while others are unable. The nurse must provide support for difficult decisions such as abortion and adoption.
Antepartum Complications in the Maternal Client
Although the majority of pregnancies are without difficulties, many are harmed by antepartum, intrapartum, and postpartum issues.
Infections
All infections are dangerous and risky for the pregnant woman and her unborn child. Some of the complications will be discussed.
HIV/AIDS
Immunosuppression in the mother can lead to the development of additional diseases, and this virus can infect the neonate both perinatally and during breastfeeding. The mother’s HIV/AIDS therapy continues, and all procedures during pregnancy that potentially raise the risk of infection to the fetus are avoided wherever possible. Episiotomy, amniocentesis, internal fetal heart monitoring, forceps births, and vacuum extractions are among the invasive procedures and interventions avoided.
Endometritis and Salpingitis
Salpingitis is an inflammation or infection of the fallopian tubes; it is most commonly caused by untreated endometritis and can progress to life-threatening pelvic inflammatory disease, severe sepsis, tubo-ovarian abscesses, and infertility.
Endometritis is an inflammation or infection of the uterine endometrium that most commonly happens after a miscarriage, spontaneous abortion, planned abortion, or as a result of another infection in the postpartum period.
Interventions may include fluid rehydration and symptomatic treatment of fever and stomach pain, in addition to the administration of antimicrobial medicines such as clindamycin or gentamycin.
Gonorrhea
Gonorrhea can also be transferred to the fetus during pregnancy and during birth. This sexually transmitted disease can cause yellowish-greenish vaginal discharge, dysmenorrhea, abdominal discomfort, and dysuria. This infection can be asymptomatic as well. Antibiotics with a broad spectrum of action, such as ceftriaxone and azithromycin, are used to treat gonorrhea.
Chlamydia
When symptomatic, Chlamydia, the most common sexually transmitted illness, can cause vaginal spotting, perineal irritation, and dysuria. Chlamydia can be treated with amoxicillin or azithromycin during pregnancy.
Toxic Shock Syndrome (TSS)
Toxic shock syndrome, which is caused by a staphylococcus aureus or streptococcal infection, can arise as a result of burns, childbirth, surgical procedures, or other forms of trauma. Streptococcal toxic shock syndrome is usually more dangerous and fatal than staphylococcal toxic shock syndrome, and the former is frequently linked with systemic collapse.
Toxic shock syndrome symptoms include hypotension, palmar desquamation, an erythematous skin rash, a high fever, altered degrees of consciousness, nausea, vomiting, and raised nitrogen and creatinine levels.
The preferred antimicrobials are first-generation cephalosporin or penicillin; however, patients who are sensitive to or allergic to these antimicrobials might be given vancomycin or clindamycin.
Hypertension
Pregnant women, like diabetics, can be harmed by pre-pregnancy hypertension, and they can also acquire gestational hypertension throughout the course of their pregnancy, which commonly begins around the 20th week of pregnancy. Pregnant women under the age of 20 and beyond the age of 40 are more likely to develop gestational hypertension than other women. Diabetes, renal disease, family history and/or a personal history of prenatal hypertension, pregnancy with multiples, the mother’s first pregnancy, and molar pregnancy are all risk factors for gestational hypertension.
Examining the Client for Postpartum Complication Symptoms
Maternal examination and care continue after the infant is delivered. These checks are conducted with the understanding that infections and bleeding are the most common postpartum problems.
The abbreviation BUBBLE is a helpful method to recall the essential components of the postpartum evaluation, in addition to the assessment of the client’s vital signs, the amount of pain and discomfort, and other assessments, during the immediate postpartum period.
The acronym BUBBLE stands for the assessment of the mother’s:
- Breasts
- Uterine fundus height, consistency and placement
- Bowel and other gastrointestinal functioning
- Bladder functioning
- Lochia amount, consistency, color and odor
- Episiotomy edema and redness
Vaginal discharge evolves from bloody vaginal drainage with occasional tiny clots for around 10 days before turning brown and lasting up to 6 weeks. Breasts are normally engorged, especially when the mother is breastfeeding; urinary output may increase during the first day or two of the postpartum period; the new mother loses about 12 or 13 pounds; and changes in hormones may lead to depressive symptoms for about two weeks, after which this depression may be serious and a sign of postpartum psychosis, rather than the “baby blues.”
Understanding Cultural Variations in Childbearing Practices
Many customers’ birthing behaviors might be influenced by culture, cultural traditions, and cultural beliefs. Some cultures, for example, value large families more than others, whilst others, such as the Chinese, limit the size of the family. Some cultures also have different attitudes about single parenthood, unmarried couple pregnancies, prenatal care, gender preference, breastfeeding, and where the infant should be delivered.
These habits and attitudes can have an impact on the importance of having children, pregnancy health practices, pregnancy beliefs, and baby feeding.
Assisting the Client with Newborn Care Performance/Learning
Moms, especially new moms and their significant others require aid and support with newborn care and infant feeding. They must understand the baby’s nutritional needs, how to breastfeed or bottle feed, cord care, and circumcision care, diapering, bonding, attachment, preventing mishaps, such as placing the infant on their back to prevent asphyxia and responding to the baby’s cries.
Nutritional Needs and Infant Feeding

Human milk is thought to be the finest kind of nutrition for infants up to the age of six months. Breast milk is produced in the breast as a result of the prolactin hormone. Prolactin, like oxytocin, is an endocrine hormone released by the pituitary gland that regulates milk production. Breast milk absorbs and digests more quickly and easily than formula milk.
A lactating breast-feeding mother’s diet should include small amounts of fat, protein, whole grains, dairy products, fresh fruits and vegetables. Special foods are not required to generate milk or to keep an adequate quantity of milk.
The typical breastfeeding process includes the infant’s and mother’s optimal positioning, latching on, and the sucking and swallowing sequence.
Positioning and holding the neonate for breastfeeding will become a personal choice, but the mother should be trained in a range of positions, including the football clutch hold position, the cradle position, the modified cradle position, and the side-lying position.
Latching on is the process of inserting the areola and a substantial piece of the breast into the baby’s mouth. The rooting response of the infant promotes latching on, and it can be encouraged by caressing the baby’s cheek while the nipple is in the baby’s mouth. The suck-and-swallow sequence begins when the infant begins to suck; the milk is then transported to the rear of the mouth with the infant’s tongue, and the infant swallows.
Cord Protection

To avoid infection, the umbilical cord stump should be handled gently and kept clean. Typically, the umbilical cord stump dries up and falls off two to three weeks after birth.
Cleansing requires the use of simple water rather than alcohol, as was formerly done. After cleaning with water, the stump should be allowed to dry naturally or with an absorbent pad. Sponge baths are preferred over tub baths, and the stump should be exposed to circulating air rather than covered with a diaper to promote drying and fall-off.
Circumcision Care
The circumcision site is maintained clean and monitored for any complications such as infection, bleeding, or a change in urinary output.
The penis is washed, coated with petroleum jelly, and then covered with a sterile dressing until it heals, which usually takes about a week.
Diapering

New mothers must also decide what type of diapers to use for their newborns until they are toilet trained. Some new mothers prefer cloth diapers, while others prefer disposable diapers. Some of the elements that may influence this decision include socioeconomic factors, the availability of a washer and dryer, and personal convenience preferences. For example, because many neonates and infants require 10 or more daily diaper changes, some parents prefer cloth diapers because the cost of disposable diapers is prohibitively expensive; and some prefer disposable diapers over cloth diapers because they do not have access to a washer and dryer and prefer the convenience of disposable diapers.
Attachment and Bonding
Bonding and attachment to the parents is vital to the new baby’s healthy growth and development. Bonding and attachments instill favorable feelings of trust and intimacy in the neonate and newborn.
Poor or absent bonding and attachments can have long-term effects such as mistrust, lack of closeness, and cognitive and psychological development problems.
Nurses can encourage both parents and siblings to hold the child, feed the infant, and converse with the infant through touch, rocking, and calming cooing sounds.
Accident Avoidance
Suffocation, falls, and strangulation are the most serious safety hazards for newborns and babies. Suffocation can be avoided by keeping all things out of the crib and placing the baby on their back rather than their stomach.
Conclusion
Everything about pregnancy is both challenging and rewarding. Some might say it was scary, yes indeed, but it is also wonderful, almost like magic seeing a human being made by love. Let’s all observe and practice the best care before and after pregnancy.
There’s a lot to learn about pregnancy and neonatal care, but no worries because AuRNPathway is offering an NCLEX course that will help you with all the things you have to learn and master.
References:
Anti/Intra/Postpartum and Newborn Care: NCLEX-RN n.d. Retrieved from
Pelvis n.d.
")
